Understanding Endothelial Dysfunction: The Missing Link in Heart Disease
By Russ Scala, Founder of Scala Precision Health
If you’ve experienced a heart attack, had a stent placed, or undergone coronary bypass—and your coronary calcium score is elevated along with lipoprotein(a)—you are dealing with endothelial dysfunction. This means the inner lining of your arteries is damaged, which is the true reason plaque forms and eventually ruptures.
Traditional medicine often follows a one-size-fits-all approach, but new research shows that endothelial dysfunction has multiple root causes. If your calcium score continues to rise year after year, it’s a clear sign that the underlying cause has not yet been identified.
Today, over 30,000 cardiologists in the U.S. largely follow the same treatment model. My goal is different: to prevent your next heart attack. After reading this, I encourage you to do your own research and understand why we may be your final option.
Back in 1996, Scala Precision Health began studying heart attacks in highly fit endurance athletes and bodybuilders—individuals with normal cholesterol levels. Despite the introduction of statins in the 1980s, heart disease has continued to rise. So we must ask: is cholesterol really the root cause?
One overlooked factor is low thyroid function, which plays a major role in heart disease. Thyroid hormones directly impact the endothelial lining, reducing nitric oxide production. Without nitric oxide, blood vessels stiffen, inflammation increases, and plaque builds more rapidly. Supporting nitric oxide is essential for both performance and longevity.
Our approach focuses on endothelial dysfunction, recognizing that each patient is biochemically unique and requires a personalized treatment plan. Many patients describe heart disease as “clogged pipes,” but that analogy is misleading. The heart beats about 100,000 times a day, and arteries constantly bend and flex. This repetitive stress damages the endothelial lining—much like wear and tear on a highway.
Calcium buildup (hard plaque) is often described as “stable,” but that’s not entirely accurate. With constant arterial movement, small fragments can break off, potentially triggering a heart attack—even in patients with moderate calcium scores.
That’s why treatment must evolve with age and be guided by advanced metabolic testing. We look deeper to identify the true cause—whether it’s insulin resistance, elevated homocysteine, hormonal imbalances, or shear stress.
What is Shear Stress?
Shear stress is the frictional force of blood flow against artery walls. In healthy arteries, smooth (laminar) flow protects the lining. But in areas where flow becomes turbulent—such as bends or branches—this stress triggers inflammation and damage, creating the perfect environment for plaque formation.
This mechanical factor is rarely discussed, yet it can initiate artery disease long before cholesterol is ever involved.
The Role of Hormones and Blood Viscosity
Certain modern treatments may unintentionally increase risk. For example, large intramuscular testosterone doses (100–200 mg) can significantly increase blood viscosity, creating abnormal shear stress and damaging arteries.
Similarly, elevated glucose and insulin levels also thicken the blood, accelerating endothelial damage and plaque buildup.
Hormonal balance is critical. Both testosterone and estrogen support nitric oxide production. Disrupting this balance—such as through estrogen blockers—can impair vascular health and increase the risk of cardiac events.
Understanding Lipoprotein(a) – Lp(a)
Early research showed that Lp(a) behaves differently than traditional cholesterol. Think of cholesterol as a large beach ball, while Lp(a) is like a small marble. When artery damage occurs, Lp(a) rushes in as a protective response—but this process can also accelerate calcium buildup.
The Bigger Picture
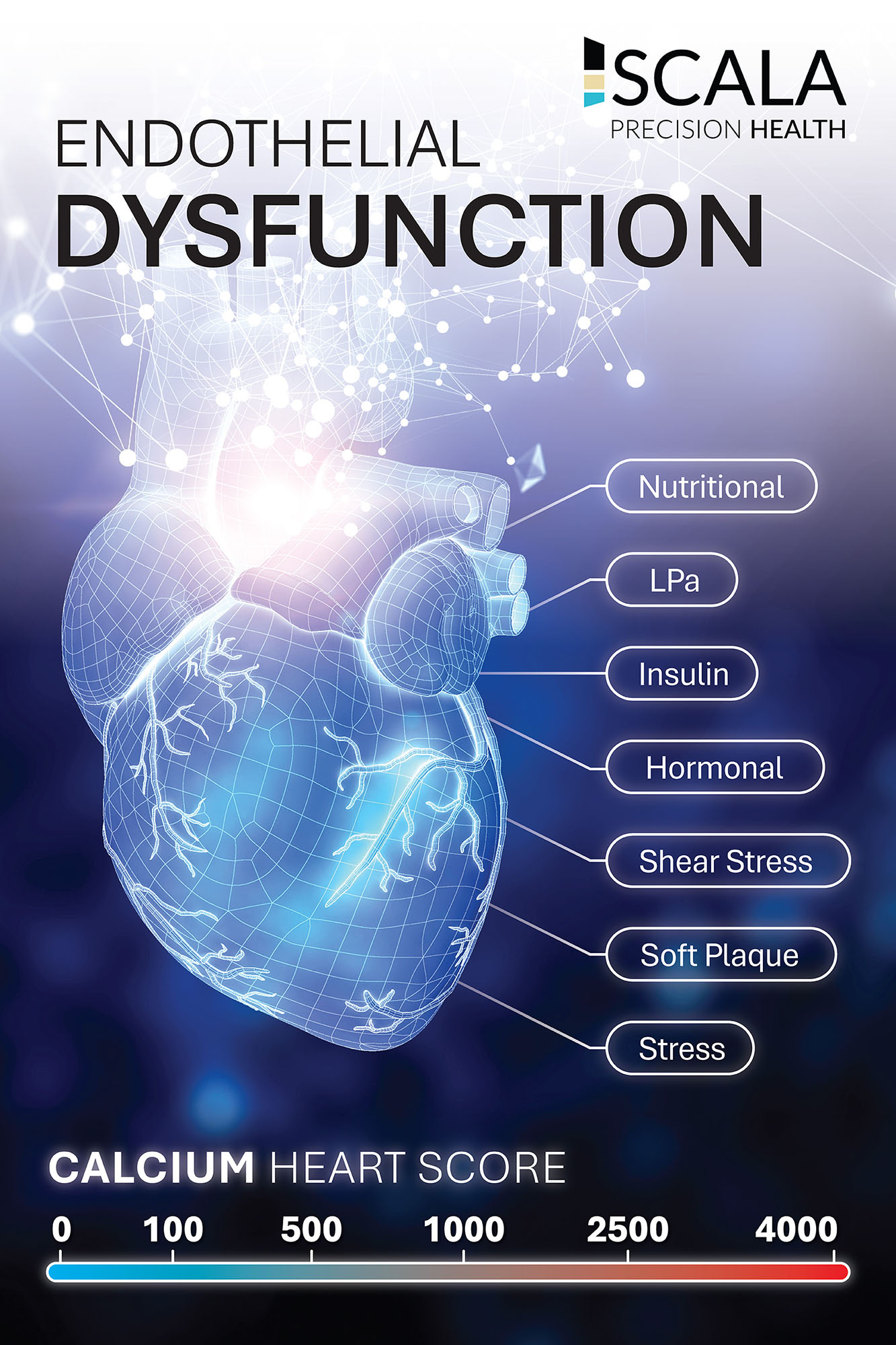
Endothelial dysfunction is driven by multiple factors:
• Inflammation and oxidative stress
• Insulin resistance
• Hormonal imbalances
• Abnormal shear stress
• Lifestyle and chronic stress
Yet, many treatment models still focus narrowly on lowering LDL cholesterol.
This disconnect reflects a larger issue: cognitive dissonance in medicine. While evidence points to inflammation and endothelial damage as root causes, outdated models persist due to years of training, industry influence, and resistance to change.
A Final Thought
Your heart beats over 100,000 times a day and pumps thousands of gallons of blood. It works harder than any other muscle in your body—yet it’s often overlooked until something goes wrong.
If you have an elevated calcium score and believe your current treatment is enough, take a step back and reassess.
Your health deserves a deeper investigation.
Want to learn more?
Visit: www.scalaprecisionhealth.com